Source: https://healthpolicy.usc.edu/article/california-native-americans-won-healthcare-settlement-federal-government-hasnt-delivered/
UPDATED MAY 03, 2021 8:44 AM
The court rulings brought hope. Finally, California’s Native American population — the nation’s largest — would receive its rightful share of federal health care funding. Triumphant, leaders in the California Native community journeyed to Washington to negotiate the process of opening the funding pipeline. That was more than four decades ago. Today, despite a 1979 federal court-ordered settlement that would have pumped millions of dollars into California for Native American health care, the state’s share remains stunningly underfunded by the Indian Health Service, Native leaders say. Their claim has been corroborated by government records and, most recently, a 2019 letter to IHS co-signed by then-senator Kamala Harris and Sen. Dianne Feinstein, urging the agency to repair “this longstanding inequity.”
The consequences for the health of the state’s largely poor and low-income Native population are incalculable. The inequitable and chronically underfunded health care services in the Golden State have driven up morbidity and mortality rates, said Mark LeBeau, chief executive officer for the California Rural Indian Health Board (CRIHB). It has cost a significant number of lives, particularly among elders. Without native elders, future generations might not have a culture and identity. “They transfer their indigenous knowledge, such as language, culture, and traditions to younger generations in their communities and this assists these young people in knowing who they are, where they come from, and what their responsibilities are,” LeBeau said. “It is critically important to provide adequate health care to these elders.” But the consequences of underfunding have also been felt by those at the opposite end of life. “A lack of funding to California Indian country has direct impacts on our youngest, our youth and upcoming generation,” Virginia Hedrick, executive director for the California Consortium for Urban Indian Health (CCUIH), said. “We already are a community that’s disproportionately impacted by poor maternal-child health outcomes.” That impact is clear at the local level, with the Urban Indian Health Institute reporting that Native babies in Fresno County die at a rate that is more than three times that of white babies. Anxious to fix this funding gap, the state’s Native leaders say one option is to go back to court in an attempt to force the IHS to fulfill the terms of the 1979 order, which found there was “no rational basis to justify” the government’s “long history of minimal funding” of health programs for Native Americans in the state. Those leaders say they’ve tried almost everything. Over the decades California’s Native leaders have testified before Congress multiple times, made pleas during numerous meetings with IHS officials, and have been involved in countless advocacy efforts. However, they say, their pleas throughout the years have been to no avail.
There are historical, economic and political reasons why California Natives have struggled to gain their fair share. It all started when a group of California-based Native Americans filed a lawsuit in the late 1970s claiming that for years Native residents had not been allotted their proportional share of federal funding for health care. By 1980, two separate federal courts had ruled in their favor after finding that the government’s own data clearly showed, in the court’s words, a “conspicuous pattern of disproportionate funding in California.” The court found that in 1977, the IHS reported the country’s Native American population served by the agency was 518,000, of which about 52,000, or 10%, resided in California. However, in the two decades leading up to 1977, data compiled by the agency showed that California had only been receiving an average of 1.18% of IHS distributions. The court also reviewed agency documents showing that the IHS had 8,100 health care workers across the country at the time of the lawsuit, but only 45 of them were working in California. The federal agency, at the time, operated 51 hospitals, 99 health centers, and several hundred health stations nationwide. California was being served by a single hospital and two health centers. The hospital has since closed. The court went on to find that the federal government had provided no argument to justify depriving the state’s Native American residents of health care services comparable to those available to Native populations in other areas of the country. “The burden of providing a rational basis for the disproportionate funding of health care programs for Indians in California has not been met,” the court concluded. “…defendants’ past and present allocation system for the distribution of IHS funds violates the California Indians’ right to equal protection of the law as guaranteed by the due process clause of the Fifth Amendment.” In 1980, the IHS appealed the decision to the U.S. Court of Appeals for the Ninth Circuit, which reaffirmed the lower court’s decision, and put the agency on notice to allocate to California its fair share of funds. “IHS was ordered to develop a reasonable, rational, distribution methodology, specific for American Indians and tribes in California, and has failed to do so,” said LeBeau, CRIHB’s CEO.
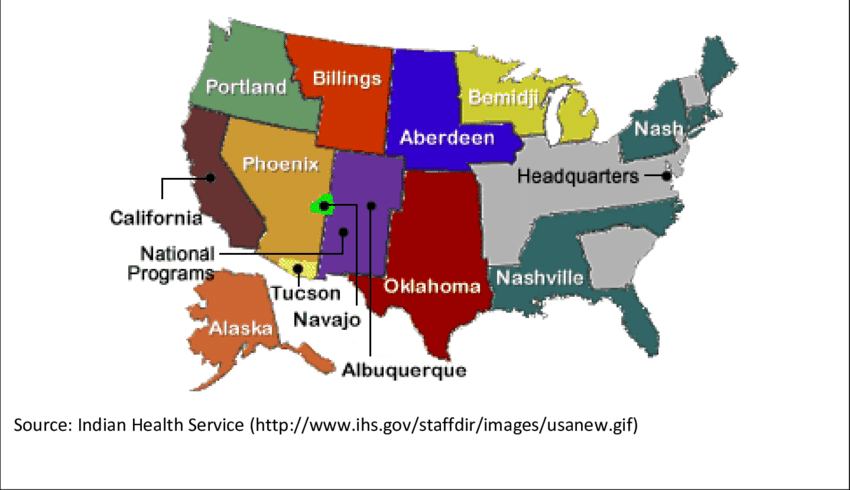
INDIAN HEALTH SERVICE AREAS
Ten regional Indian Health Service offices, in addition to Navajo and Tuscon offices in Arizona and a national headquarters in Maryland, oversee contracts with providers to American Indians and Alaska natives across the U.S.

After World War II, according to a 1986 Congressional review of IHS, the federal government ceased providing health services to California’s Natives. It wasn’t until 1970 that the state asked the federal government to resume those services. But by then, California was substantially behind other states in obtaining IHS funds. It has received lower funding ever since. CRIHB was one of the organizations established by Native leaders in 1970 to bring back IHS services to California, according to the review. Beverly Miller is director of the California Area IHS. When asked what IHS has done in the last 40 years to address the underfunding of health care programs for Native Americans in the state, she acknowledged “there are some things that have not changed over the years.” Among them, Miller said, is a “shortage of human and financial resources and the challenges of providing care in the most remote corners of the country.” While she said there are no IHS hospitals in California (the agency operates 24 in the other 11 areas, plus 51 health centers), she said Congress recently funded two youth regional treatment centers. One of them is in Hemet, and provides services to youth ages 12 to 17. The other center is in Davis and is expected to open later this year, Miller said.

Read more at: https://www.fresnobee.com/news/local/article250797364.html#storylink=cpy
AN UNDERFUNDED AGENCY Miller left little doubt that the agency is inadequately funded. According to figures provided by Miller, in the year 2017, IHS spent $4,078 per capita, compared to a U.S. national health expenditure the same year of $9,726 per capita — more than twice as much. The agency’s budget for fiscal year 2020 was $6.0 billion. After the 1980 court ruling, leaders from California traveled to Washington, D.C., where they met with Congressional leaders and encouraged them to fairly allocate funding, LeBeau said. It is Congress that appropriates funding for the Indian Health Service, which then allocates the money to its 12 areas throughout the country. California is one of those areas. Several organizations, such as the CRIHB, California Consortium for Urban Indian Health (CCUIH) and the National Indian Health Board “have been fighting this fight for 30 years or more,” said CCUIH’s Hedrick. “We just need a government that is ready and willing to respond.” But Native Americans in California continue to be deprived of services that other IHS areas across the country enjoy, leaders say. “We are just essentially advocating to be underfunded at the same level as tribes in other IHS areas across the country,” LeBeau said. “We’re very financially poor in receiving IHS funding in California, and we just want to be brought up to being as poor as our colleagues in other IHS areas across the country.”
The agency currently only receives enough funding to cover 60% of the health care needs of Native Americans across the country, according to the agency’s website. “We’re really handing out breadcrumbs,” Hedrick said. The July 2019 letter sent to IHS by then Senators Harris and Feinstein says that over 39 years independent authorities have determined Native Americans in California receive a substantially smaller portion of IHS outlays than they deserve. The court required the IHS “to adopt a program for providing health services to Indians in California which is comparable to those offered (to) Indians elsewhere in the United States,” the letter points out. However, they say in the letter, a 2012 report from the Government Accountability Office found Indians in California were still not getting their fair share of federal funding, and there were no IHS hospitals in the state, despite California being home to more Native Americans than any other part of the country. “We urge you to develop a plan to remedy this longstanding inequity,” Harris and Feinstein wrote. Inquiries to Harris, who is now vice president in the Biden administration, went unanswered by her office. Adam Russell, a spokesperson for Feinstein, said the senator continues to work on the issue.

POLITICS AT THE IHS Jessica Farb, director for the Health Care Team at the U.S. Government Accountability Office, said the 2012 GAO report reached the same conclusions that the senators did. But while IHS implemented some of the GAO’s recommendations, others were not adopted, Farb said. Some of that failure, Farb pointed out, is due to internal politics among the tribes. “IHS provided information to GAO that made it clear that IHS would not be able to make changes that reduced funds to any tribe,” Farb said. “It is our understanding that this is a very sensitive issue with the tribes.” According to a Congressional report from the ‘80s, even at that time, it wasn’t “surprising” that there was “great reluctance” to redistribute base budgets among the various IHS areas across the country. Inquiries on this matter to the office of Health and Human Services Secretary Xavier Becerra, whose agency oversees IHS, went unanswered.

LACK OF AN INDIAN HEALTH SERVICE HOSPITAL IN CALIFORNIA
Meanwhile, California has the largest Native American population in the nation, with around 720,000 residents, according to the U.S. Census. The state is home to about 100 reservations or rancherias. But, again, it has no IHS hospital. Charles D. Fowler, chief executive officer at Central Valley Indian Health, Inc, said Native Americans in California are at a “major disadvantage” compared with their counterparts in other states, given that lack. “There’s absolutely nothing on the horizon saying that there’s going to be a hospital here in the state,” he said. “It would certainly be a benefit to the Indian people in California.”
As a result, inpatient care is not available through the Indian Health Service in California. Patients who need to be admitted to a hospital, or need to see a specialist, have to be referred to providers in the community, Fowler said. But the IHS budget for referred care in the state is “grossly underfunded,” Hedrick said. That shortage of funding forces Native American patients in California to seek care outside the IHS system and apply for health insurance through Medi-Cal, the state’s insurance for poor and low-income residents, or through the Affordable Care Act.
ANOTHER EXAMPLE OF NATIVE AMERICANS IN CALIFORNIA BEING LEFT BEHIND
The inadequate funding coming to California from IHS has forced tribes to borrow, seek donations and apply for grants in order to “cobble together” enough dollars “to fulfill the Indian Health Service’s responsibility to provide care for tribes in California,” LeBeau said. “When you think about that, IHS is obligated to provide health care to tribes in California,” he said. “They haven’t provided the clinics, they haven’t built those facilities, to me that’s a very important issue that needs to be addressed.” Another IHS program has failed the state’s natives. Under the 1991 Joint Venture Construction program, LeBeau said, if a tribe or a consortium of tribes can find money to build a clinic and it is approved by the agency, IHS will cover the cost to staff it for 20 years. Tribes in California have submitted multiple applications over the years, LeBeau said, but only one has been approved. Since the program’s inception, the agency has funded at least 35 projects, including five in 2020, according to the IHS.
LACK OF COMPLIANCE WITH 1980 COURT ORDER
LeBeau and others have testified before Congress on multiple occasions, most recently in 2018. At this juncture, LeBeau said, he doesn’t know what direction his organization will take. “We are doing our due diligence to exhaust all avenues, and certainly the potential of having the court now do a review of the level at which IHS has complied with its order,” LeBeau said. Dorothy Alther, an attorney and executive director for the California Indian Legal Service, which was involved in the original legal action, said the suit was before her time, but she is intimately familiar with the issue. Alther has sued over the inadequacies of funding to tribal law enforcement, and she relied on Rincon, as the 1979 case is known, “quite heavily.” What the courts have found, she said, is that if Congress appropriates money to a federal agency without guidance on how to spend the money, the court can’t review how the agency chooses to allocate it. “The law in this area is not good,” Alther said. Support for the reporting of this story was provided by First5LA. Story direction was provided by The Center for Health Reporting at the University of Southern California’s Schaeffer Center for Health Policy and Economics.
This story was originally published May 2, 2021, 5:00 AM.